My previous essays laid out the current situation with healthcare in this country. Assuming that research will continue to provide new treatments, techniques, equipment, diagnostic tools, and medications, we can expect the costs of healthcare coverage to grow faster than inflation.
What can we do?
In this note I will list a group of suggestions that, I believe are attainable within the political limits of where we are today.
There are 332 million citizens in this country.
We spend $4.9 trillion on healthcare.
This represents a spend of $14,750 per citizen.
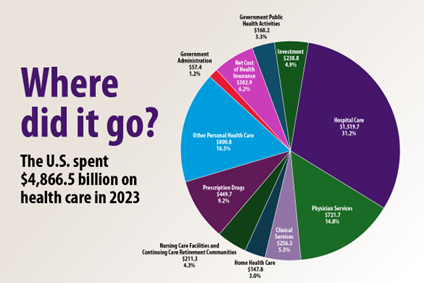
Of the money spent, about 30% goes to hospital care, 20% goes to physicians and clinical services, and 10% goes to prescription drugs.
Hospital care is the largest pot of the most money spent on healthcare per year, accounting for 31.2% of spending, followed by physician and clinical services (20.1%) and retail prescription drugs (9.2%).
In the US:
22% are under 18
36% are between 18-44
25% are between 45-64
18% are 65 and over
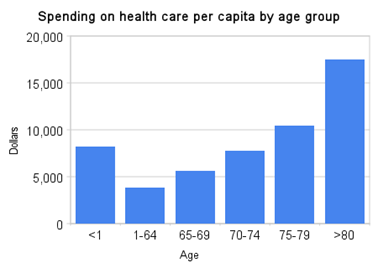
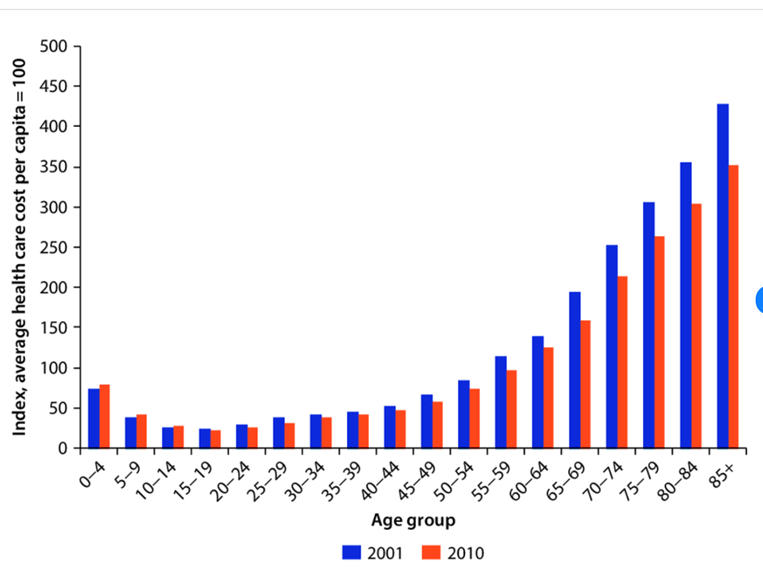
Most healthcare expenses occur at the beginning and end of life. Children under 1 year have double the costs of those between 1 and 64; and people over 80 have 5 times the cost of that same population.
68 million citizens are covered by Medicare including 61 million who are over 65, and 7 million who are under 65 but have disabilities.
80 million citizens are covered by Medicaid (an additional 24% of the population)
Of these, 37 million are children (representing almost 50% of all children), and includes both Medicaid and CHIP (the Children’s Health Insurance Program).
Together, Medicare and Medicaid cover the healthcare insurance for about 43% of the US population.
FIRST SUGGESTION: PEDIACARE
Perhaps we could create a program that would piggyback on the current Medicaid and CHIP programs to expand government run health insurance for ALL children under the age of 5. This would expand the universal coverage by and additional 10%.
Pediacare could consolidate Medicare for children, CHIP and the new group of children under the age of 5 into a single program.
Since the administrative infrastructure already exists, there should be a relatively easy transition to this program. There would be only a slight incremental increase in people to run this expanded program. Economies of scale, the ability to negotiate with providers based on the single payer, large group model, and integrated records would provide better care. Insurers would be relieved of one of the age cohorts that costs the most and therefore should be able to reduce their premiums.
Pediatric care has healthcare (and therefore financial) benefits throughout life. The major causes of adult morbidity and mortality begin in the early years of life. Obesity, diabetes, mental, emotional, behavioral and substance abuse disorders have all been shown to correlate with pediatric health.
I would add some responsibility requirements to this program. For example, we might require that there be at least 2 pediatric examinations per year to maintain Pediacare coverage. It is the responsibility of the parents to ensure that their children not only ARE covered, but that they USE that coverage. The program needs to be a two-way street. Parents must protect their child, and the insurance must protect the parents.
Pediacare could also require adherence to societal healthcare needs. For example, I would include the requirement that all children be vaccinated against childhood diseases. Not only do these diseases cause financial strain due to hospitalizations and deaths, but they put other citizens at risk. Another example is including a requirement for seeing and hearing screening tests to catch health issues at the earliest possible time. This will decrease long-term effects as well as long-term costs.
SECOND SUGGESTION: CRITICALCARE
21st Century Healthcare has provided us with treatments that were never imagined 50 years ago. Transplants of a wide variety of organs, long-term maintenance of previously mortal diseases like Cancer and AIDS, and surgical solutions to heart, lung, and brain conditions that would have caused death in the past are now commonly used. But these interventions are expensive.
A cornea transplant costs $34,000; A kidney transplant averages almost $500,000; a liver transplant $1,000,000; a lung transplant about $1,900,000, and a heart transplant about $2,000,000.
Overall, the total costs for transplants in the US are around $30 billion per year, which is less than 1% of the total spend on healthcare.
Managing a cancer patient can cost hundreds of thousands of dollars including chemotherapy, radiation, surgery and ongoing medications.
The total costs for cancer services in the US are around $200 billion per year, which is about 4% of the total spend on healthcare.
Brain surgery costs are high because of the surgery, ongoing care, rehabilitation and therapy. They can reach $1,000,000.
The total spend on Brain injury and treatment in the US is about $40 billion per year, which is less than 1% of the spend.
Heart or lung surgery can range from $30,000 to $200,000.
Perhaps we can incorporate coverage for all of these “Critical” healthcare conditions into the current Medicare Program under a program called “CriticalCare”.
As with the idea of Pediacare, this program would assume the financial management of these procedures, developing economies of scale, better rates through negotiation with providers, and a savings in premium costs for the public.
The total funding of CriticalCare would be a little less than $300 billion, which is about 6% of the total healthcare spend.
THIRD SUGGESTION: AI HEALTHCARE RESEARCH FUND
AI will transform many industries; healthcare will be high on the list.
Imagine that you are wearing a Smart Watch, or Smart Ring, or Smart Bracelet. Each is equipped with sensors to determine your vital statistics like heart rate, blood pressure, blood oxygen, blood sugar, EEG, body temperature, stress hormones, etc. These pieces of technology will have the ability to recognize changes in your health status, they will have the ability to connect to a centralized clearinghouse and to notify your healthcare provider. In emergencies they could contact rescue organizations or ambulances and notify a hospital of your status.
Combine that technology with an AI “SmartDoc”, and a partnered pharmacy and the speed of treatment can be accelerated dramatically.
The net result is that conditions that today could result in catastrophic incidents, could be caught in time, resulting in better outcomes, and far less expenditures.
I would like to see this possibility accelerated, and government-funded research into this would not only provide that accelerated development, it would also provide a public program that would not be controlled by private for-pay systems that would compete with each other for dominance and standardization but would increase costs.
HOW TO PAY FOR THESE PROGRAMS
There is no free lunch.
Programs cost money.
Even if those programs result in less expenditures overall on healthcare, they still require funding. Even if they result in lower premiums that offset, or save overall spending for consumers, the government will need to cover those costs.
And it is a truism that no matter how much money is saved by the insurers, and how much they are able to (forced to, see the MLR), that savings will disappear over time as regular inflation, and healthcare cost escalation take affect.
So, how do we fund these new programs?
One of the funding issues with the current system is that the cost to the consumer for healthcare insurance coverage is based on per capita costs. Each person covered pays the same regardless of their financial position. I believe that a progressive tax would be a more equitable way to pay for these programs; programs that would cover the entire population and result in increased health, better ability to work, increased productivity, increased presenteeism, and decreased stress on the system in general.
What would we need?
Based on the numbers above, we would need
$540 billion for the expansion of coverage to include all children in PediaCare.
$330 billion for CriticalCare.
$ 50 billion for AI Smart Health research and implementation.
Or, a total of $920 billion.