
The media has become obsessed with the numbers of new cases reported each day. In this case Mr. Trump is mostly correct. The more tests you do, the more cases you will identify. That is just a mathematical fact. It takes a little more analysis to understand those numbers. I will have a little more to say on this issue later this week in my end of October report.
I have always insisted that looking at case numbers is not particularly valuable. Instead I always focus on deaths.
However, there is another statistic that has some value – Hospitalizations. Although these numbers are not as reliable as deaths, they have significantly more value than cases. And one of the ways you can use that data is to look at how deaths in hospitals relate to the numbers of people hospitalized.
This comparison is made in the attached graph.
In order to make a fair comparison you need to look at how many people, on average are hospitalized each week and then compare the number of deaths that occur 2 WEEKS LATER. This is because the majority of deaths occur 14 days after hospitalization. That is not to say that some people don’t die quickly, because they do; nor is it not to say that some people remain in the hospital for months before they succumb to the disease. That is why a fair estimate of death is 14 days.
The graph plots the deaths as a percentage of hospitalizations since July 1.
Remarkably, the mortality using this method has remained quite constant during the entire period with an average of 50.3%.
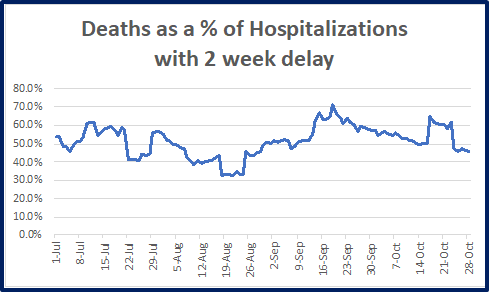
This analysis suggests that we have had little success in decreasing mortality of this disease, although there seems to be downward trend in mortality since the middle part of September.
Some caveats to that statement:
First, we don’t know if the criteria for admission to the hospital has changed over time. For example, if we now are admitting only patients who are more severely ill than before, then a maintained mortality rate would actually mean improvement.
Second, therapeutics. Therapeutics should reduce some aspects of hospitalization, but not necessarily lethality. A good example is remdesivir, which has not shown a decrease in mortality, and has only shown improved outcomes when used early and when measured as days spent in the hospital. Dexamethasone may be effective, but the data has not yet been clear on reduction in mortality statistics.
People who are admitted to the hospital may spend a few days, a few weeks or a few months. It therefore becomes exceedingly difficult to correlate hospitalizations with positive case identifications.
The best estimate is that over the period since May 1, there have been about 466,000 people in total hospitalized. Over that same period there were 8,700,000 positive cases identified. If these numbers are correct, then hospitalization represents about 5.4% of the total cases identified. Using a lethality of hospitalized patients of 50.3%, that translates to an overall lethality for ALL positively identified patients of 2.7%. We can assume that this estimate is a little bit high since we are still limiting testing to people who either have symptoms or who have been in direct contact with someone who has the virus. This is why estimates of actual infections is some multiple of the 9 million currently identified. Please remember that the lethality for influenza is 0.1%, so even if the COVID-19 estimated lethality is off by a factor of 2, the lethality of COVID-19 is about 14 times higher.