
In Colorado the Pine Beetle has been devastating large areas of Pine forests. As those forests die out, the Colorado Aspens have been growing and replacing those areas with new growth. In the future, as the Pine Beetle dies out, new pine trees will take hold in those Aspen forests. Because Pine trees grow faster than Aspens, they will begin to retake those areas and in the future the Aspens will be replaced by new Pine forests, and the cycle will start anew.
This is normal evolution; the faster growing trees will supplant the slower growing ones.
The same phenomenon is seen throughout the animal and plant kingdom, and we are now seeing it in the COVID-19 world. A new variant has emerged that apparently has a higher transmission rate. In England and in South Africa, where it has established itself in the community, it is replacing the original strain. We can be totally certain, 100%, that the same strain has already been seeded in the US. It is only a matter of time before that strain becomes the primary strain in this country, so it is valuable to understand how this occurs, what it means and what effects it will have on our population, treatments and vaccinations.
WHY IS THERE A NEW VARIANT?
Please understand that this will not be the last variant to emerge; others will develop over time. This is not because the virus is “intelligent”; it does not know what it is doing. Mutations in the viral genome occur when the genome is replicated, because the system is not perfect. A lot of mutations in the genome, when they happen, are lethal to the virus. Those mutations might occur in the RNA strand in an area that is responsible for replication, and the resultant variants do not replicate and die out. Some of the mutations may occur in the proteins that are involved in getting the virus into the cell or causing the mRNA to be replicated. If the mutations allow the virus to enter the cell faster, or make more copies, it will become more transmittable and more dominant. If, the mutations prevent entry or slow down replication, those variants will not appear in the population as they would be dominated by the current strain.
If the mutations occur in the spike protein, in the part of the protein that creates the basic structure, they will likely have little effect. However, if the mutations occur in the binding region of the spike protein, AND they allow the spike protein to bind more strongly to the cell surface, that strain will begin to replace the existing strain. Finally, if the mutations allow the virus to infect additional types of cells, for example in the upper respiratory tract rather than just the lower respiratory tract (as the current strain does), then quicker infection and higher virus shedding loads will be seen and the virus will become more dominant.
As we spoke before, the mRNA has a series of “codons”, groups of 3 bases, each of which codes for a specific amino acid in a protein chain. A point mutation in one of these 3 bases in a single codon would result in the replacement of one amino acid in a protein chain with a different one. (There are other types of mutations, but let’s keep this simple for now). Sometimes this mutation is lethal to the virus, sometimes it is neutral and sometimes it is advantageous. The advantageous mutations will become more dominant.
There have been 17 mutations identified in the new variant.
Some of these mutations occur in areas of the RNA that have no identified functionalities. This is not at all unusual. There are large sections of the genome in RNA viruses, DNA viruses and even our own chromosomes whose function is unknown. There may be some use that we simply do not understand; there may be no function at all, because over time mutations have occurred in these sections that make them non-functional and are simply carried along as excess baggage, and there may be some sections that were functional in species that preceded the current one and are no longer needed much like software programs that have replaced older versions may still carry along older sections of code that have now been either inactivated or overwritten.
7 of these 17 mutations occur in the spike protein. Some occur in the binding area of the protein allowing for stronger binding to the cell and some occur in the structural area of the protein. Of these, there are a few that occur in the area of the protein chain to which the Lilly monoclonal antibodies bind. At this time there is no information as to whether those variations will prevent the monoclonal antibody therapeutics from being successful.
WHY WILL THIS VARIANT BECOME DOMINANT?
The new variant may bind better to cell receptors, making it more likely to infect the cells, and if mixed with the older strain, it might be the first one into the cell.
It appears that the new variant may infect the upper respiratory tract, which is less common in the older strain. This might give the variant a head-start in infection, and it may lead to faster virus shedding and higher shedding amounts.
Some reports have suggested that the new variant is 70% more transmissible. This is probably the most important factor and I will discuss the implications below.
WILL THIS VARIANT CAUSE A DIFFERENT DISEASE?
Not very likely at all. These mutations and variants are quite normal, most of these individual variations have been seen before. It is very difficult to determine the severity of disease as so many people have sub-clinical symptoms, but most experts believe that there will be no significant changes in the severity of disease with the new variant.
WILL VACCINATIONS STILL WORK?
This is probably the most common question, and again, most experts believe that the vaccines will still work. The immune response activated through the presentation of the spike protein is wide enough that even if a small part of the protein is modified, the balance of the protein will remain the same and even if there is a small subset of antibodies that no longer recognize the spike protein, there will still be plenty of antibodies stimulated to prevent infection.
WHAT IS THE EFFECT OF HIGHER TRANSMISSIBILITY?
In a previous essay I spoke about “herd immunity” as related to the infectivity of the virus. Right now, with the current virus, experts think that we need to reach a vaccinated population equal to about 70% of the total population. If the transmissibility increases, that threshold will also increase, probably to about 80% of the population. The main effect of higher transmissibility is the need to increase the percent of population vaccinated.
HOW WILL WE REACH THOSE PERCENTAGES OF VACCINATIONS?
I particularly like the adage: “Vaccines will not prevent disease, vaccinations will.”
Here is a graphical representation of how long it will take to reach 70% or 80% immunizations. I have made several adjustments in order to arrive at these numbers.
First, I have assumed that there are currently 30 million people in this country who have been infected with and who have recovered from the infection. This is about twice the reported number of identified cases since testing began.
Second, I have assumed that these infections, yielding “natural” immunity will continue to occur at the same ratio of population as has been before. Those numbers will decrease as the population becomes immune through either infection or vaccination. I use these numbers to supplement the vaccinations in order to reach the levels of herd immunity.
The results are shown below.
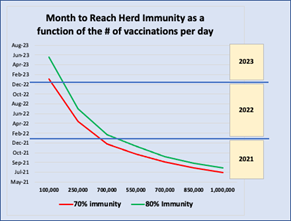
Here are the take homes:
(Right now, we are administering about 150,000 doses per day. That translates into 75,000 vaccinations per day since the vaccine requires 2 doses, about 3-4 weeks apart.)
First, if we only immunize 100,000 people per day (200,000 doses per day), it will take until January of 2023 before we reach 70% immunity in the US population.
Second, if we reach 1 million people per day, we can reach those levels by the summer of 2021.
CAN WE REACH VACCINATION LEVELS?
The problem today is that in the US we have shipped a little over 11 million vaccine doses since December 13 (13 days), but we have only administered a little under 2 million vaccinations, or about 150,000 doses per day.
There is no clear indication of why those additional 9 million doses have not been administered.
- There may be a shortage of staff able to do the vaccination
- The distribution has been left to the states and we don’t know how well the states have planned
- Each patient is required to wait in the location for 15 minutes after the immunization in order to watch for any allergic reactions and this may slow down flow-through.
- There may be some issues in contacting those people who are eligible for vaccinations.
Whatever the lag is, if it is not resolved we will have difficulties in reaching herd immunity levels before the end of 2021.